Before starting with this article I think it is important to remind you that the following lines are not a class nor are they intended to be a guide on decompression for my dear divers friends who do the favor of reading me, this exercise is just an attempt to show in a simple and basic some concepts about the dynamics of pressurized gases and decompression that sometimes tend to be confusing or complicated, if you want to learn decompression, gas mixtures and, as they say, the “black arts” of diving, there are formal courses that you can take with many instructors who are geniuses in this alchemy of gases, saturation and pressure.
First of all, I think it is important to specify the importance of assuming that regardless of the level at which we are practicing this wonderful sport, this is a personal decision and we must be aware that we decide to practice an activity with multiple potential risks that have a very short response time. . Assume that the day they became divers they agreed to interact with marine life in the wild, that divers get lost, that divers suffer from decompression, that divers have accidents.

It is your responsibility to stay updated, in healthy physical shape and to continue training and practicing the skills learned in your courses.
I recommend that you do not forget these fundamental principles:
- Never put yourself above your training level.
- Never be a “cheap diver” when it comes to training and gear.
- Be a diver aware of your surroundings when diving, on the boat, and with all the risk factors that exist in this activity.
- It is your responsibility to have health insurance that covers diving.
- Every dive must become practice of some skill, no matter how insignificant it may seem; throwing the buoy without being necessary, practicing buoyancy, becoming aware of breathing, navigation and any other learned skill must be practiced consistently or it is forgotten.
- My personal philosophy is to take a course and specialize in something different related to diving each year.

ACCIDENT ANALYSIS
When talking about decompression it is always good to keep in mind some interesting facts about diving accidents. Most diving accidents are a combination of factors that trigger the accident, and if they are addressed in isolation, they can be stopped and thus prevent its development. Diving accidents rarely occur suddenly.
MAIN CAUSES
- Lack of proper training.
- Inappropriate gas management.
- Bad buoyancy control
- Gear malfunction, in bad shape or in need of maintenance.
- Confined spaces.
- Environmental conditions.
- Preexisting medical conditions.
Diving casualty data published in Diving Medicine for Scuba Divers in (2015)
- 90% died with their weight belt on.
- 86% were alone when they died (diving alone or separated from their buddy).
- 50% did not inflate their buoyancy compensator.
- 25% got into trouble on the surface.
- 50% died on the surface.
- 10% were in training when they died.
- 10% who were not medically fit to dive.
- 5% were cave diving.
- 1% of rescuers died.
Ten recommendations from DAN to pay attention and be able to make safer dives.
- Proper weight.
- Good buoyancy control.
- Extra attention to gas planning and management.
- Ascent speed control.
- Use of pre-dive checklists.
- Attention to dysbaric injuries.
- Have a better cardiovascular health.
- Dive more often (or more refresher training before trips).
- Increased attention to diving within personal or training limits.
- Less equipment /proper maintenance issues.
Please friends, diving with regulators, BCD and diving equipment that are 20 years old does not make you more intrepid and tough divers, it only puts you at risk, the diving equipment wears out and has a useful life, "even if it's still working ”. Renew your diving equipment constantly and please get rid of your wetsuits and “vintage” equipment, they are simply not safe.
Decompression Theory
Decompression theory appears to be a complex web of scientific terms, laws and complicated processes written in ancient Chinese-Mandarin that often leaves divers wondering why on earth they thought it would be a good idea to learn more about decompression?
- The researchers and scientists who currently study it are the first to admit that we know very little about it.
- It is a fascinating part of diving that underpins everything we learn to try to be safer divers.
- Try to go beyond the recreational limit of diving and you basically become a lab rat for decompression research.
A common mistake among recreational divers is to think that decompression theory is a well-understood process, that we know everything there is to know about decompression in diving, and that simply by “following the most conservative computer or “boards” will avoid developing decompression sickness (DCS).

To understand a little about this wonderful process of decompression, it is necessary to go back a little in time to understand the origin of the theory of decompression developed by John Scott Haldane (1860-1936), a Scottish physiologist and biologist.
- This friend, in the early 1900s, commissioned by the Royal Navy, began studies on inert gas saturation in living beings that are subjected to breathing gases at more than 1ATM pressure.
- It was a precursor to the first compressed air diving tables, which describe the process of nitrogen absorption by the body when breathing it at high pressures.
- Haldane suggested that we consider the body as a group of tissues that absorbs and releases gases at different rates and in order to explain these observations, he proposed four basic principles:
1- The absorption and elimination of gas in a tissue occurs exponentially.
2- Different tissues absorb and release gas at different rates.
3- Decompression is achieved by decreasing the ambient pressure.
4- The tension of a gas in a tissue should not exceed approximately twice the ambient pressure.
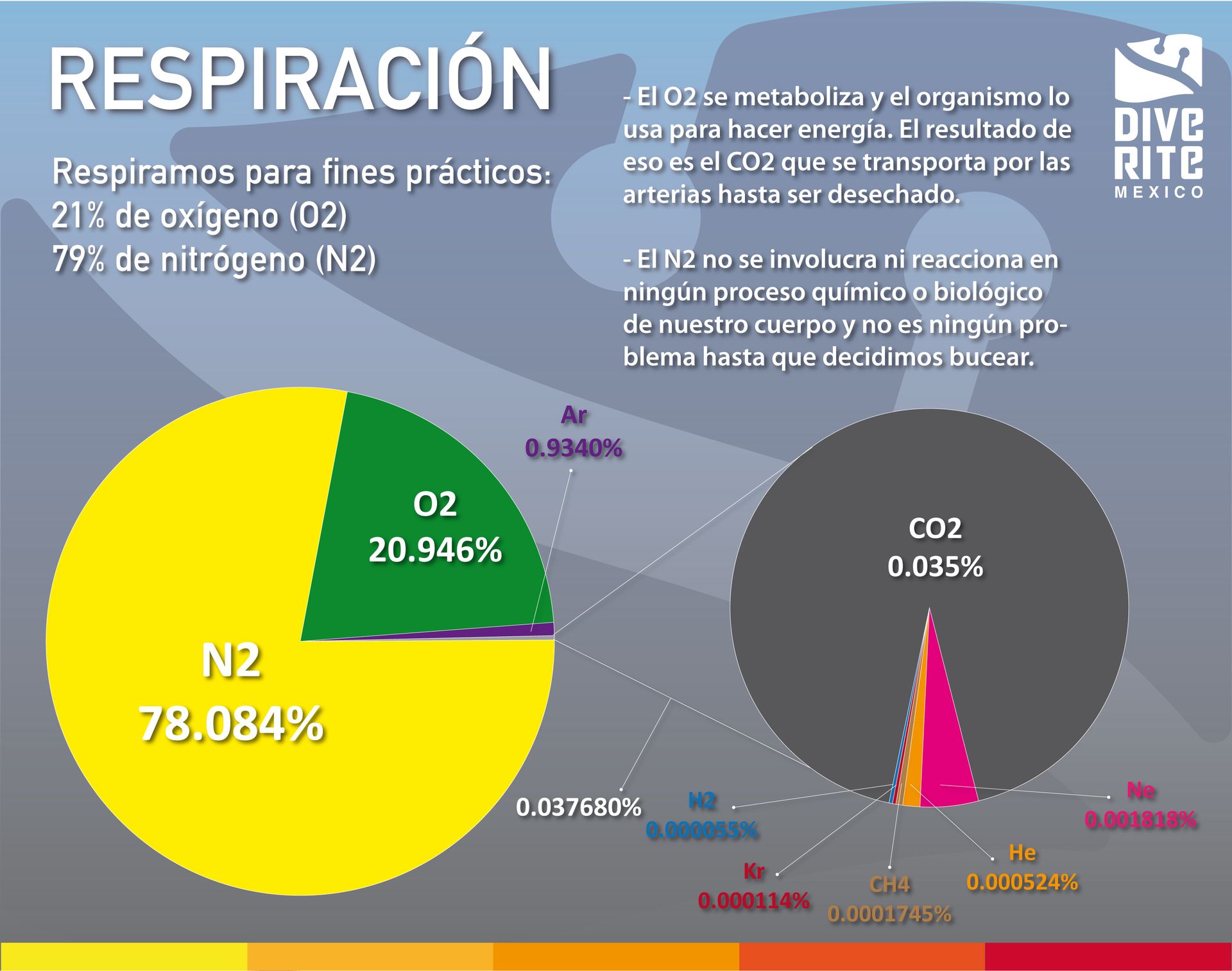
To better understand decompression, let's start by establishing what we are breathing and what function these gases play in our metabolism.
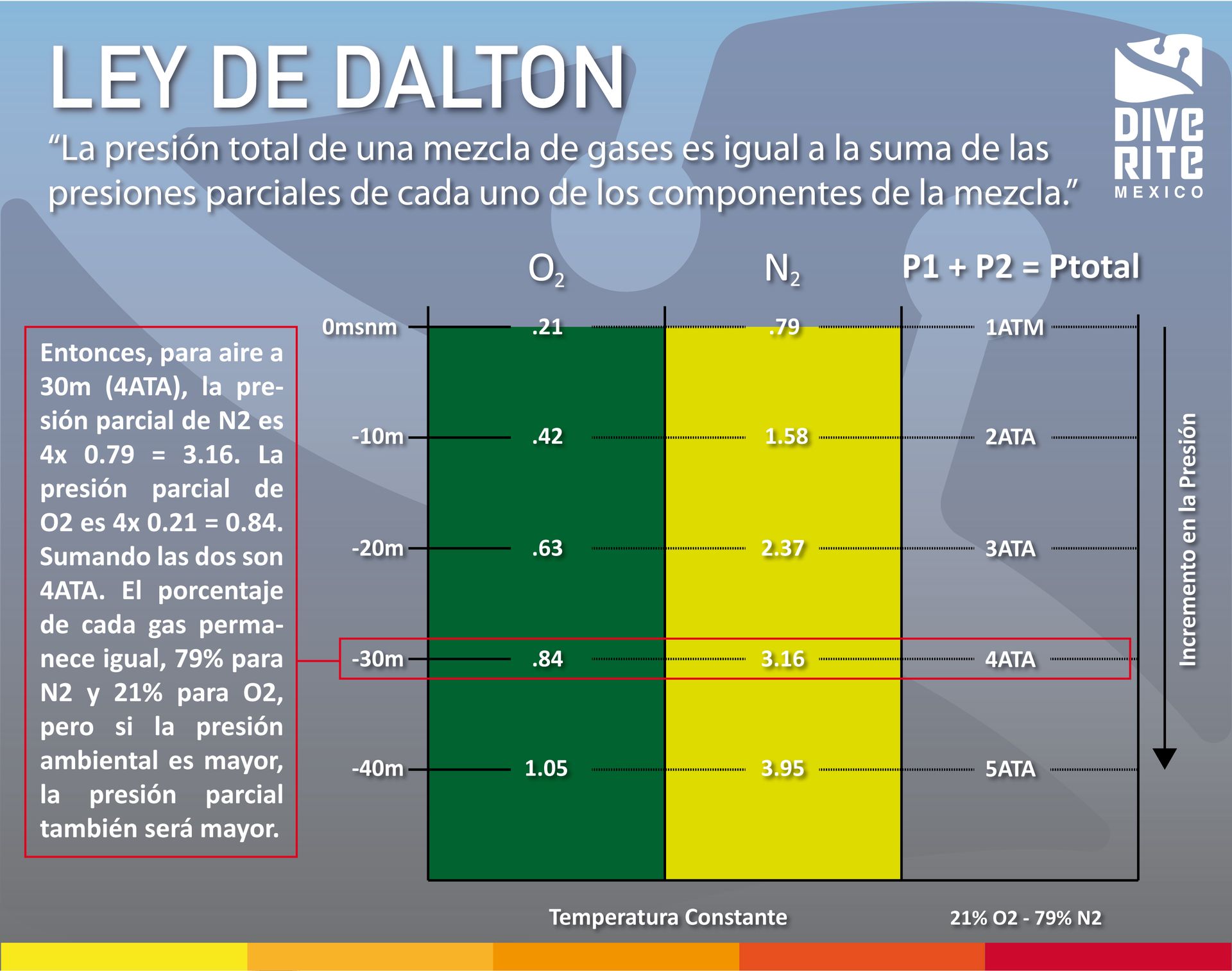
Now we have to understand a little better 3 gas laws that are involved with this decompression process.
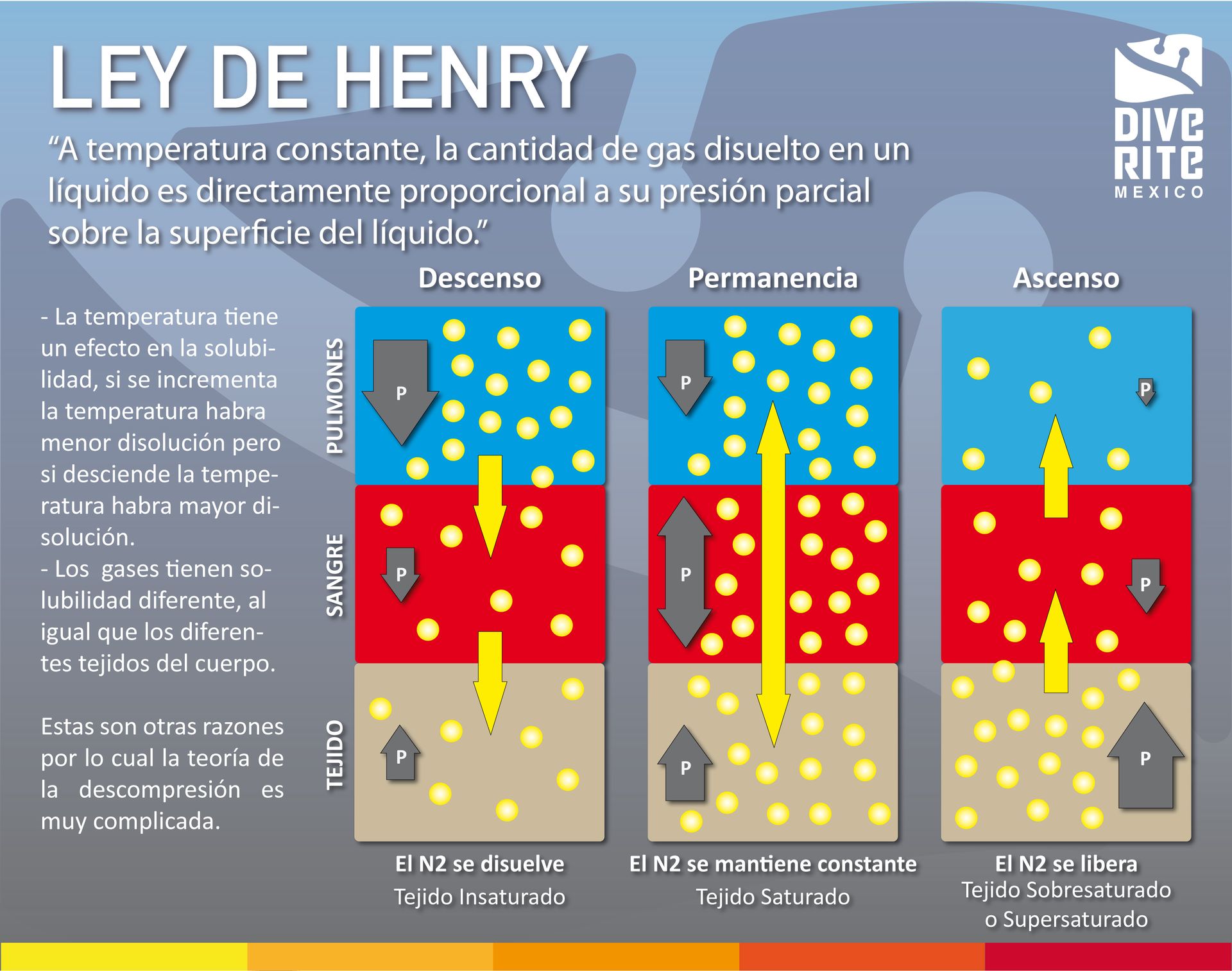
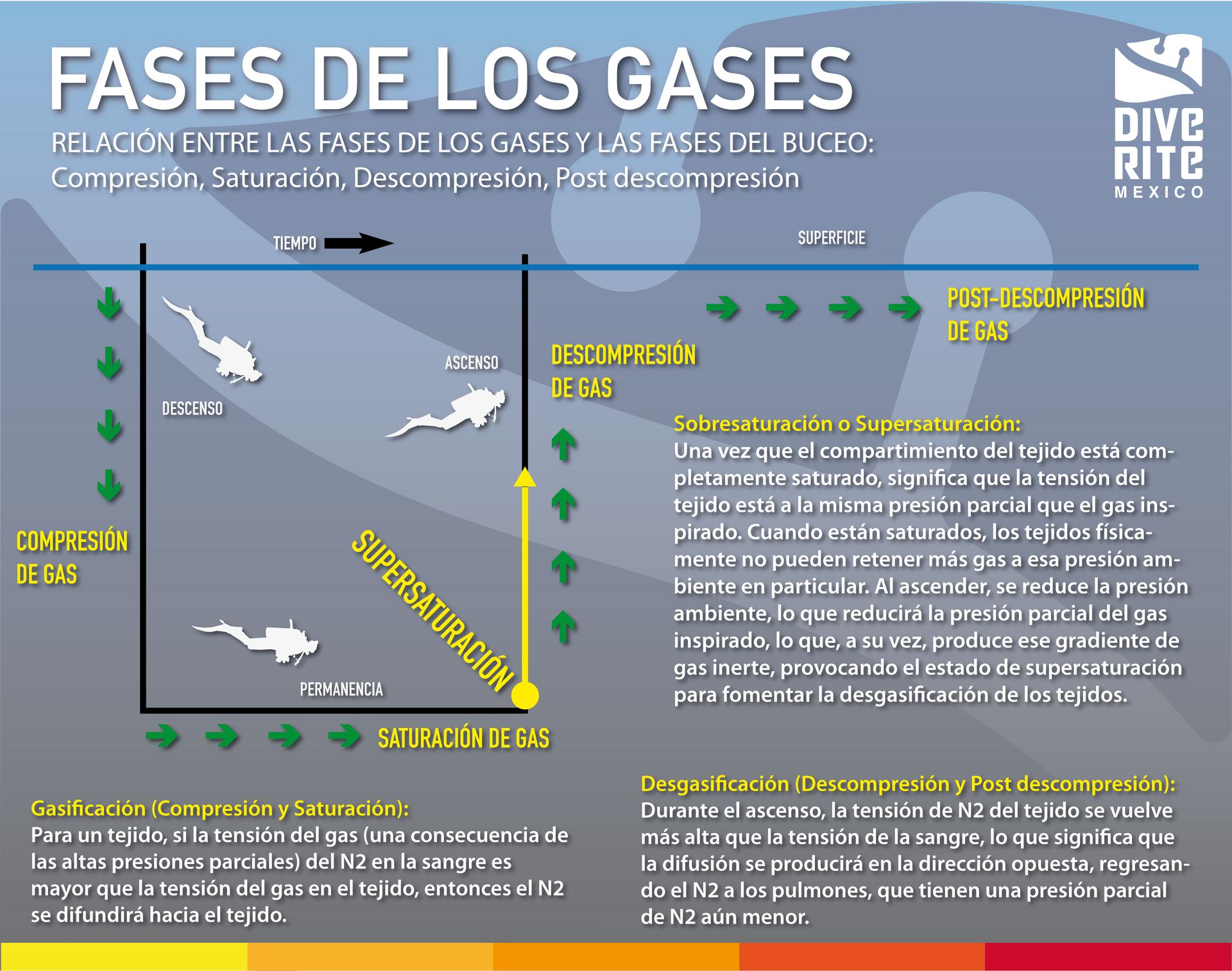
It is important to mention that there is a RELATIONSHIP BETWEEN THE PHASES OF THE GASES AND THE PHASES OF DIVING, that is; Each phase of diving that we know as descent, permanence, ascent and interval on the surface corresponds to a phase of the gas called compression, saturation, decompression and post-decompression, that is, depending on which phase of diving we are in, we are affecting the gas. inert gas that we breathe in a direct and specific way and it is important to understand this to have clarity when we are diving about what is happening with the inert gas involved in our diving.
N2 SATURATION
In the process of saturation of inert gas (in this case N2) in diving, several fundamental factors are involved that will affect the amount of gas that the organism will saturate, such as: diffusion, perfusion and tension. gaseous. On the other hand, we have that the composition of the body's tissues also influences the process of gas saturation and desaturation. Here I give you a clearer definition of each of these factors.
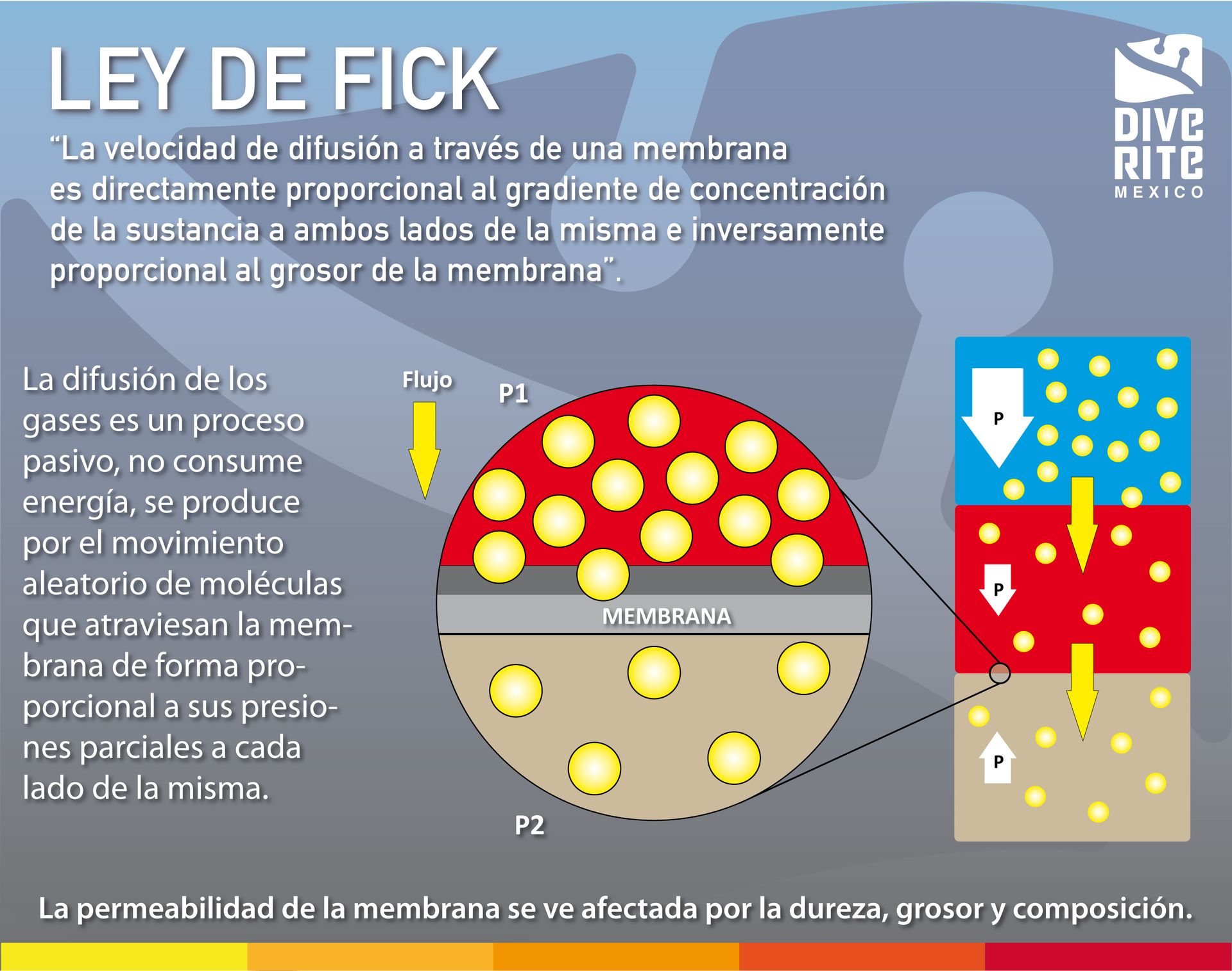
Diffusion: (simple) It is a process by which a flow of molecules occurs through a permeable membrane without there being an external supply of energy. In this process, the movement of molecules occurs following the concentration gradient; Molecules cross the membrane from the medium where they are in higher concentration to the medium where they are in lower concentration.
Perfusion – Basically means blood flow, or the rate of blood flow. Blood moves around the body, moving gases from the lungs and transporting them to smaller and smaller capillaries, until these capillaries become only one cell thick, allowing oxygen to reach the tissues.
Gas tension: Liquid and gas interface. The gas exerts pressure on the liquid because its (gas) molecules exert an attraction or repulsion on the molecules on the surface of the liquid. But it is very small because the gas has a very weak density in relation to the liquid.
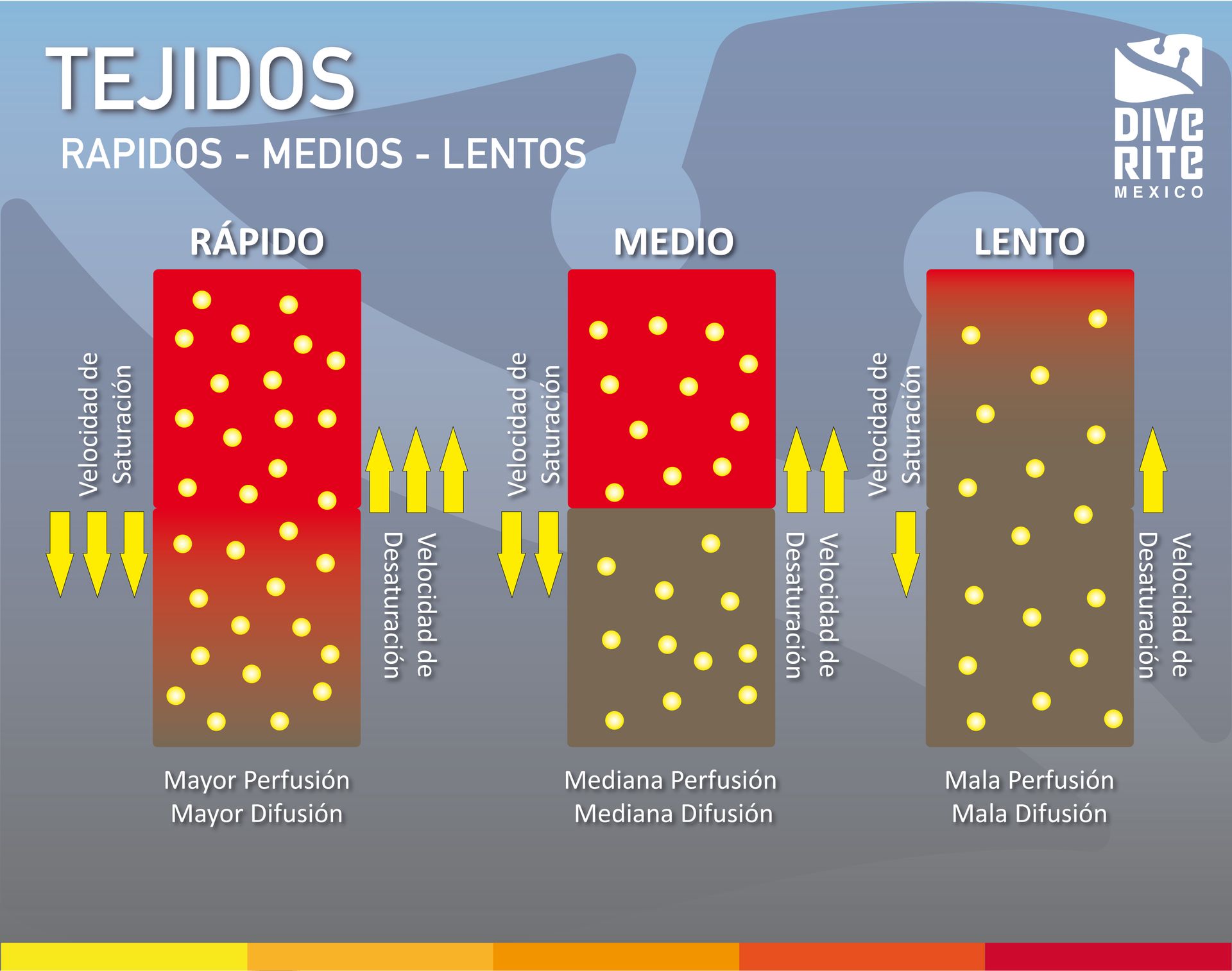
Fast, Medium, and Slow Tissues (Tissue Compartments): Tissues are defined as fast, medium, or slow depending on the combination of tissue perfusion and diffusion. Different tissues in the body are supplied with blood at different rates. Brain, blood, heart, and muscle are well perfused and have good diffusion, while bone, fat, and cartilage are more poorly perfused and have poor diffusion.
I understand that saturation is a mathematical calculation and that therefore there is a "constant" in the following graph I show you the so-called average times that Haldane proposed to calculate the saturation of the gas.
Half Times: Haldane was the first person to test and model what happens to the body during a dive, proposing that so-called tissue compartments be used to model different body tissues. He used 5 compartments, all with different “half times”.

(Half time is a general scientific term most commonly used in radioactivity.) Describes the time it takes for a radioactive material to decay to half the original number of atoms. But it can also be applied to gas absorption, and for a given tissue compartment it means the time it will take for it to become half saturated with inert gas.
While it is likely that during recreational diving a fast tissue compartment can saturate, slower compartments will not, unless you aim for a bottom time of 450 minutes to saturate the 75 minute tissue (compartment 5).
La gráfica a continuación ilustra lo que está sucediendo entre la presión inspirada de N2 (que estamos respirando) a cierta profundidad y la tensión gasesosa (entra o sale gas del tejido) y cómo cambia dependiendo de en que fase del buceo nos encontramos.
The M-Values or maximum values are limits that are established to prevent the loss of ambient pressure from being too much, causing the gas that is dissolved in the tissue to go into a gaseous state, causing decompression sickness in the diver. This graph is an explanation. of the relationship between M values and ambient pressure.
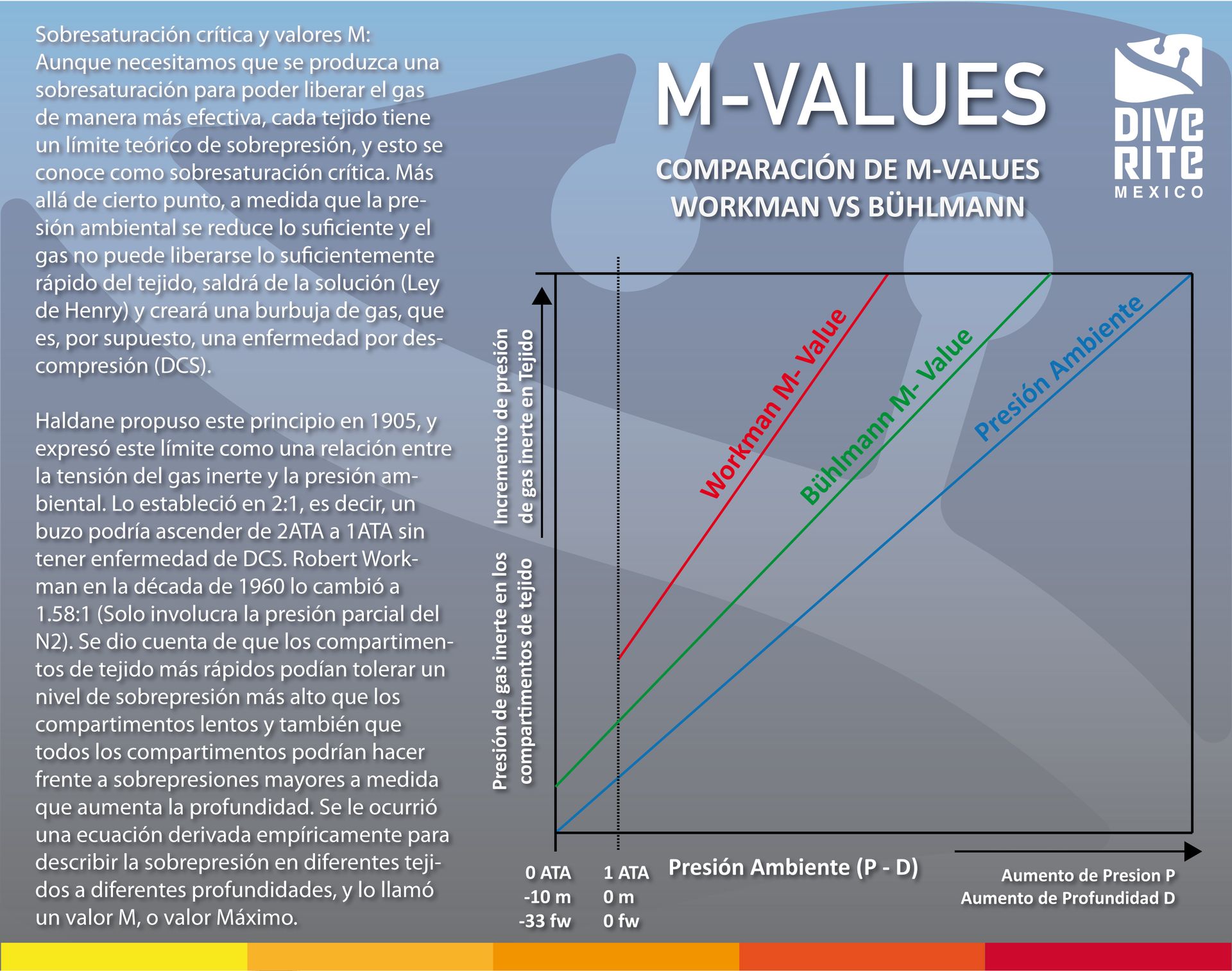
- The variables that control whether tissue pressures remain within the M value are depth, time and rate of ascent. Greater depth means greater gradient of inert gas between our lungs and our tissues, which means more gas can enter solution. Longer bottom times mean more time to saturation, which, conversely, means more time required to degas on ascent.
- Recreational divers are largely concerned with fast tissues and LNDs (limits of no decompression). The depth limits are designed to avoid excessive gas loading on slower tissues. These limits, combined with the maximum ascent rates, mean that divers can make a direct ascent to the surface and remain within the M value for the main tissues (those closest to the M value).
To conclude this section I leave you a little about the silent bubbles that play an important part in the decompression equation and are another factor to take into account during our dives.
Silent Bubbles: In 1976 a report was published on the detection of so-called silent bubbles in the bloodstream of divers. They were not bubbles causing DCS, the bubbles were found in divers who were not showing symptoms, and who had all dived very conservatively and within the limits of the diving tables of the time.
- Further research on these silent bubbles suggests that they may be permanently present in the bloodstream, even for people who have never dived. This is due to a combination, of a mechanical nature, of cavitation, micro-nucleation and tribonucleation.
- Silent bubbles are now considered a completely normal consequence of diving. However, it is very difficult to correlate the size and frequency of silent bubbles with DCS cases. Some people fold with few or no silent bubbles and others have no symptoms of DCS even though they have what is considered an excess of silent bubbles.
To continue trying to complicate (I say clarify) things further, it turns out that today we have different gas saturation models that contemplate and calculate differently what is happening with the inert gas in our body. The gas saturation models used by dive computers today, although in practice they have some similarities, actually rely on quite different issues to calculate LNDs or decompression stops. When we dive in a group with friends, it is common for us to have similar LNDs between various types and brands of computers and the variations are usually minimal, the recreational diving industry has standardized parameters, limits and standards that make it appear that dive computers calculate incorrectly. the same way, but it is not true.
Find out from your dive computer what algorithm it uses and that you use in particular to calculate LNDs and how many compartments are used in that algorithm, (hint…it comes in your computer's manual).
Let's talk a little about the models we have and what they are based on to make gas saturation and desaturation calculations:
Characteristics of dissolved gas models or also called classic models:
- Calculate the dissolved gas.
- The model can be perfusion controlled or diffusion limited.
- Gas exchange is controlled by gas perfusion and diffusion.
- Inert gas exchange is driven by the local gradient, the difference between arterial blood and local tissue tension, and they seek maximum loading or removal.
- Elimination is maximized by shallow decompression phases.
- Diffusion dominates in tissues with minimal vascularity and greater distance between capillaries.
Features of free phase gas models:
- Calculate the gas separated in the free phase.
- The model is controlled by perfusion.
- The gradient of removal of inert gas from the bubbles increases with depth.
- Reduce pressure gradually to minimize bubble formation.
- Deep stops are designed to maximize free phase gas removal.
- Deep stops decrease the total decompression time in a free phase model compared to a dissolved gas model.
They all still use the concepts of mean times and M values for dissolved gases, but also try to model bubble size and shape as they are subject to different pressures over the course of a dive. Explaining how they do it involves talking about the complicated mathematics and mechanics of bubbles. But in simple terms, we know that a bubble has several different forces acting on it. It has external environmental pressure, surrounding tissue pressure, and its own surface tension. All of these forces are interacting in a way that will determine whether or not the gas will diffuse into the bubble and make it larger, or diffuse and shrink. If a bubble reaches a certain size, it is believed to have reached the so-called critical limit, which could mean it could become a symptomatic bubble. The objective of these models is to keep the bubble below this critical volume.
There are several different and variable models to choose from: Bühlmann ZH-L12 - ZH-L16, US Navy, DCIEM, DSAT (PADI), Variable Permeability Model (VPM), Reduced Gradient Bubble Model (RGBM), etc…
To complicate it even more, there is another factor that we have to talk about and that even today is (although less and less) a little confusing due to the number of options that exist and are called “Decompression Rates”. ascent” that affect everything that has to do with the different phases of gases during a dive, M values, amount of supersaturation, size and quantity of silent bubbles, vary depending on who you learn to dive with..
Ascent speed limits depending on who you ask:
- BSAC 15 m/min (up to 6 m)
- SSI 9 m/min
- PADI 18 m / min
- Paul Bert recommended 3 m / min
- Haldane recommended 1.5-9 m / min
- Bühlmann 10 m / min.
No one seems to agree on what the ideal rate is, or even whether there is a single ideal rate. In 1958, the United States Navy revised the promotion rate for Navy divers. They wanted a climb speed of 30m/min, but the divers thought this was too fast for them carrying heavy equipment, so it was set at 18m/min.
Most instructors and divers sensibly do not climb faster than their computers allow (9-10m/min). For decompression dives, the common practice is that from the bottom of the dive, through the deep stops to the first decompression stops, 9m/min is the maximum (and also the minimum), then to the stop At 6m the ascent speed is 3m/min. From 6m to the surface it is 1m/min.
MY RECOMMENDATION IN RECREATIONAL DIVING IS 9-10m/min and from the safety stop to the surface 1m/min.
Let's talk a little about decompression sickness, a pathology associated with diving that is under constant study and that cannot be seen as a static phenomenon that only happens to certain divers under specific circumstances. The reality is that things continue to be discovered about decompression, its origin and evolution. Decompression sickness is a sum of factors combined and added to the biology and individual characteristics of the subject who develops the disease; Therefore, the only thing we can do to try to avoid it is to pay attention to the factors that contribute to its development to try to avoid them and reduce the risk of developing it.

Hablemos un poco sobre la enfermedad por descompresión, una patología asociada al buceo que se encuentra en estudio constante y que no se puede ver como un fenómeno estático que soló le sucede a ciertos buzos bajo circunstancias especificas. La realidad es que se siguen descubriendo cosas sobre la descompresión, su origen y evolución. La enfermedad por descompresión es una suma de factores combinados y sumados a la biología y características individuales del sujeto que desarrolla la enfermedad; por lo tanto, lo único que nosotros podemos hacer para tratar de evitarla es poner atención a los factores que contribuyen a su desarrollo para intentar evitarlos y disminuir el riesgo de desarrollarla.
PREVENTION
- Training.
- Diving with nitrox is recommended.
- Hydration.
- Understand and use tables, computers and saturation algorithms.
- Good health and physical condition.
- Sleep well.
- Do not use tight wetsuits.
- Do not exceed the no-decompression limits.
- Do not do strenuous exercise underwater.
- Do not exercise after diving.
- Do not bathe with hot water.
- Do not drink alcohol or coffee in excess during the diving period.
- Do not undergo diving with thermal stress.
- Do not sunbathe.
- Do not carry out any activity that could activate the gas.
CONCLUSION
Friends, as you can see, the issue of breathing inert gas under pressure results in a question between science, religion and alchemy. There are many things that we still have to discover. I hope that these graphs and small conceptual explanations that I made will be of help to you. to understand a little better the fascinating world of gas saturation and desaturation that happens during diving.
To summarize....
- Compartments and M values are a mathematical way of trying to imitate biological processes. The human body is too complex to model accurately and there are too many factors that do or do not contribute to tissue gassing or degassing. Bins and M values are the best GUESS we have, no more, basically algorithms are a leap of faith.
- Millions of people dive every year without incident, so they seem to work in some way, but we don't know for sure what is really good and what is not, since it is very difficult to conduct studies on divers that give subjective responses to questions about diving profiles that are not precisely controlled. Controlled studies in large groups of divers of the type that could produce statistically relevant results simply do not happen.
- Formal training and practice is the best way to prevent diving accidents.
- Albert Bühlmann's work continues to be used in most dive computer algorithms..
- Comparing saturation models always helps to make better decisions for safe diving planning.
- Finally, the fact that we have different algorithms, dive tables and ascent rates only demonstrates how uncertain are our attempts to model the effects of gas saturation and desaturation on living organisms with individual characteristics and complex biology.
Safe Diving!
RICARDO CASTILLO M
Recreational and technical diving instructor
Nº. 386 NSS-CDS (National Speleological Society)
Nº. 13580 SDI (Scuba Diving International)
Nº. 13580 TDI (Technical Diving International)
Nº. 8308 IANTD (International Association of Nitrox and Technical Divers)
Nº. 339806 PADI (Professional Association of Diving Instructors)
Nº. 14919 DAN (Divers Alert Network)